 E-Submission
E-SubmissionPubMed Central, CAS, DOAJ, KCI

Articles
- Page Path
- HOME > J Yeungnam Med Sci > Volume 40(Suppl); 2023 > Article
-
Resident fellow section: Teaching images
Ultrasound-guided diagnosis/intervention for ischiofemoral impingement syndrome -
Wei-Ting Wu1,2
 , Ke-Vin Chang1,2,3, Levent Özçakar4
, Ke-Vin Chang1,2,3, Levent Özçakar4 -
Journal of Yeungnam Medical Science 2023;40(Suppl):S134-S136.
DOI: https://doi.org/10.12701/jyms.2023.00500
Published online: July 12, 2023
1Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Bei-Hu Branch, Taipei, Taiwan
2Department of Physical Medicine and Rehabilitation, National Taiwan University College of Medicine, Taipei, Taiwan
3Center for Regional Anesthesia and Pain Medicine, Wang-Fang Hospital, Taipei Medical University, Taipei, Taiwan
4Department of Physical and Rehabilitation Medicine, Hacettepe University Medical School, Ankara, Turkey
- Corresponding author: Ke-Vin Chang, MD, PhD Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, Bei-Hu Branch, No. 87, Nei-Jiang Rd., Wan-Hwa District, Taipei 108, Taiwan Tel: +886-2-23717101-5309 • E-mail: kvchang011@gmail.com
Copyright © 2023 Yeungnam University College of Medicine, Yeungnam University Institute of Medical Science
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
- 949 Views
- 74 Download
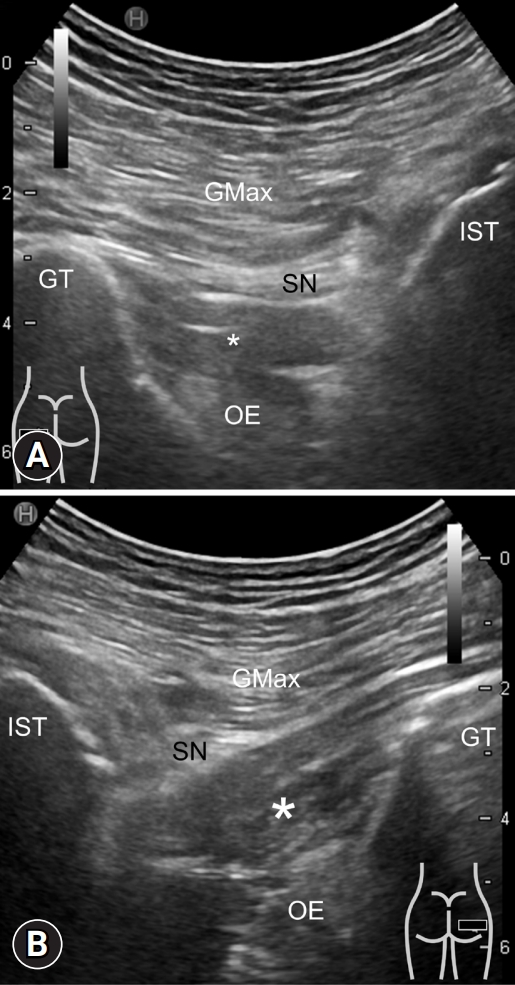
- • Ischiofemoral impingement syndrome is caused by narrowing of the space between the ischial tuberosity and trochanter, leading to posterior buttock pain.
- • Magnetic resonance imaging is the gold standard for diagnosis, whereas ultrasonography can help visualize the deep gluteal muscles.
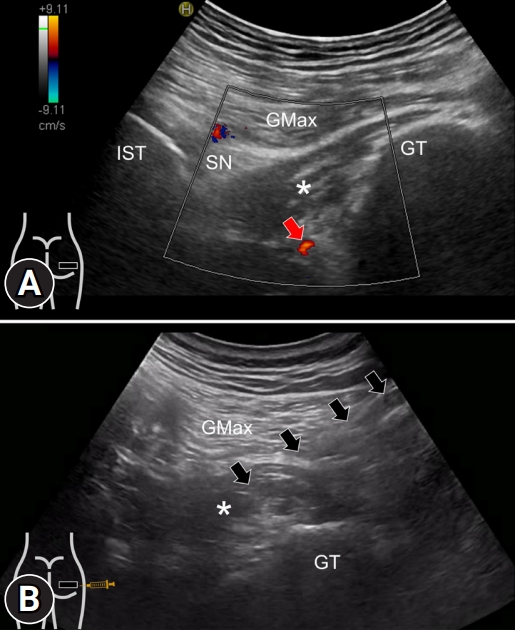
- • Ultrasound-guided injection between the quadratus femoris and obturator internus is useful in treatment but requires power Doppler imaging to prevent collateral vascular injury.
Learning points
-
Ethical statements
In the authors’ institutions, approval from the institutional review board is not required for the case report. Written patient consent was obtained for the publication of this report.
-
Conflicts of interest
Wei-Ting Wu and Ke-Vin Chang have been editorial board members of the Journal of Yeungnam Medical Science since 2021. They were not involved in the review process of this manuscript. There are no other conflicts of interest to declare.
-
Funding
This work was funded by the National Taiwan University Hospital, Bei-Hu Branch; Ministry of Science and Technology (MOST 106-2314-B-002-180-MY3 and 109-2314-B-002-114-MY3); and the Taiwan Society of Ultrasound in Medicine.
-
Author contributions
Conceptualization: all authors; Investigation, Data curation: WTW, KVC; Formal analysis, Funding acquisition, Supervision: KVC, LÖ; Validation: LÖ; Visualization: KVC; Writing-original draft: KVC; Writing-review & editing: all authors.
Notes
- 1. Wu WT, Chang KV, Mezian K, Naňka O, Ricci V, Chang HC, et al. Ischiofemoral impingement syndrome: clinical and imaging/guidance issues with special focus on ultrasonography. Diagnostics (Basel) 2022;13:139.ArticlePubMedPMC
- 2. Scorcelletti M, Reeves ND, Rittweger J, Ireland A. Femoral anteversion: significance and measurement. J Anat 2020;237:811–26.ArticlePubMedPMCPDF
- 3. Gómez-Hoyos J, Martin RL, Schröder R, Palmer IJ, Martin HD. Accuracy of 2 clinical tests for ischiofemoral impingement in patients with posterior hip pain and endoscopically confirmed diagnosis. Arthroscopy 2016;32:1279–84.ArticlePubMed
- 4. Akça A, Şafak KY, İliş ED, Taşdemir Z, Baysal T. Ischiofemoral impingement: assessment of MRI findings and their reliability. Acta Ortop Bras 2016;24:318–21.ArticlePubMedPMC
- 5. Chang KV, Wu WT, Lew HL, Özçakar L. Ultrasound imaging and guided injection for the lateral and posterior hip. Am J Phys Med Rehabil 2018;97:285–91.ArticlePubMed
- 6. Mezian K, Ricci V, Güvener O, Jačisko J, Novotný T, Kara M, et al. EURO-MUSCULUS/USPRM dynamic ultrasound protocols for (adult) hip. Am J Phys Med Rehabil 2022;101:e162–8.ArticlePubMed
 PubReader
PubReader ePub Link
ePub Link Cite
Cite


